@DunningKruger I recognise sarcasm when I see it and I understand your frustration at having to use it, but sometimes it's the only way to bring out the awfulness of a situation.
In England, I got a retinal detachment. I went to a high street optician at 3pm that day, who diagnosed the condition for free using computer scans. They told me I needed to go immediately to the hospital. I was seen by a surgeon at the hospital two hours later. He told me he was going to operate the next morning. At 8am the following morning, I was operated on by a specialist eye surgeon (an Iraqi) and a younger colleague who looked like a movie star. The procedure lasted an hour and a half. You're awake throughout it all, I could see everything, including a suction drill inside my eyeball.
I recovered for two hours at the hospital with free tea and biscuits. I went home and had four follow-up checks over the next four months, which included numerous different eye scans and two sets of eye medication. The eye is fixed and all is well. They saved my sight. There was no invoice, there was no check on my financial situation. I shook the surgeon's hand and thanked him. He said, "It was my pleasure."
@Richard65 In America, we pay ridiculous insurance premiums for not “all inclusive” coverage. Surgeries can go into the hundreds of thousands. Imagine if you only had 80% coverage after deductible? And that’s common…The average single person probably pays $135/wk for health insurance.
That’s roughly $7,000/yr. A family plan is roughly double the cost. If you come from somewhere like the UK to here, health care is a real head scratcher.
The more you look at it the more it raises questions.
I can believe the general point but not the massive death-rate; and it does not define "health insurance" hence the "lack of" it.
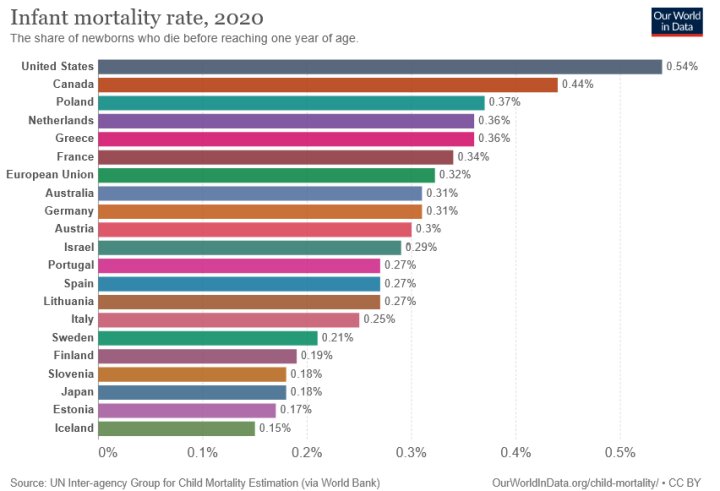
I assume the diagram is from someone somewhere trying to tell us the USA offers only commercial health services, with no national health service as operates in so many other nations. So, the same unknown source is presumably trying to tell us many (really, nearly half a million?) Americans die each year because they cannot afford medical insurance or treatment.
I thought the USA does have a very basic national service for the very poorest who cannot afford hospital fees, but I don't know its extent and details. Also, we'd know relative situations of preventative medicine, health education and ways of life, for any such statistics to mean much.
All the countries named including the USA have "health insurance" of some sort; whether commercial, State welfare services or as in the UK, both. Where only commercial health services are available they are not affordable to many people; or some who can afford it remain untreated by falling foul of insurers' exclusions designed to minimise pay-outs, hence maximise profits.
Also, the numbers quoted look suspiciously exact for a mean value of many high numbers, but may only be by simple, purely-arithmetical rounding to an integer. More importantly, over how many years have the statistics for all those nations been examined; and factors such as the Covid pandemic accommodated?
Thirdly, what of other factors that will influence untimely fatalities by illness; such as relative natures and levels of preventative medicine, health education and ways of life? What if of two countries of similar levels of health provision and costs-of-living, the residents of one live fairly abstemiously on reasonably good diets but those of the other largely neglect themselves?
This could affect commercial health cover. An insurer's primary task it to make money not make people well; so may well charge higher premiums or even exclude those who limit their own lives by being under-nourished, over-weight, hard-drinking smokers. Would such cases - the needless premature fatalities by heart-attacks etc. - therefore bias the "lack of insurance" claim, by the insurance existing but excluding those people?
What are the sums based on? Genuinely no insurance, commercial or state? Or insurance existing but too expensive or exclusive for many people?
That diagram alone seems based on either very poor statistics or good statistics badly handled or even wilfully misreported.
It would be interesting to read the source so we know what it is really trying to say. I don't suppose the source is a medical-insurance company...?
@jshm2 everyins. plan is different, all depended on where you worked, i worked in a union factory, my insurance will cover me no matter what country i am in, just like i was home in usa, for same co-pay of $15, but no many people have that that kind of ins, if you met 100 people from different states, every one will have a different kind of insurance, medicare for people over 65, might barely be the same, on just a few
According to the office of national statistics 130,641 deaths occurred in the UK from treatable or preventable illnesses in 2021/2022. Our population is pretty small compared to the US
I wonder how much the figures are also affected by typical life-styles and relative levels of health education in simple disease avoidance, as well as practical or financial availability of treatment once illness occurs.
@ArishMell it all DEPENDS ON WHERE YOU WORKED, all government jobs have good ins. teachers all good, unions all good, if you are on welfare, they get everythng free, no could barely talk english, it depeded on where you worked, my ins, is free, i cost my ins. company 140K, last year, i paid $600, pretty good
In countries like the UK and many others, you can take out private medical insurance and/or pay singly for private treatment, if you can afford it; but otherwise the State system pays for national's medical care irrespective of occupation, unemployed or retired; or union membership.
There are some exceptions. Here, we pay towards opticians' and dentists' services even as National Health Service patients (the private fees are a lot higher) and until aged 60, part of the cost of prescription medicines. That fee goes to the NHS not the pharmacists, who have to sell "over-the-counter" medications, personal care products and cosmetics for their own income.
There are also certain exemptions, if on particular State benefits other than the State Pension: though retired I still need pay towards my dental treatment and spectacles.
That is the UK so the details will vary from country to country but the basic model is the whole system is funded from general taxation, not by the public hospitals and general-practioners invoicing their patients.
It was initiated in the late-1940s thanks to Aneurin Bevan, the Labour MP who saw the problems among his South Wales, industrial-area constituents on very low pay, studied the mutual-assurance plans that had evolved among them to help pay doctors' fees, and thus created the foundation for the National Health Service. Originally he intended it being fully "free at the point of use" but the government quickly realised that was not going to be sustainable so introduced the Prescription Fees to help with the cost of medicines.
....
Most European countries have similar systems, and these are given reciprocal arrangements so visitors between them can receive treatment if they fall ill during their stay. The home welfare system re-pays the host's service.
@ElwoodBlues BTW, malpractice insurance is frequently cited as a driver for our high medical costs. It causes some increases, but by no means all.
Most malpractice suits occur in state courts. States like Texas passed malpractice reforms in the early 2000s, yet their medical costs still match the rest of the nation. See https://www.nber.org/aginghealth/2009no3/w15371.html The authors found that tort reforms had minimal effect on premiums of fully-insured plans.
Furthermore, according to https://www.forbes.com/sites/stevecohen/2015/03/02/on-tort-reform-its-time-to-declare-victory-and-withdraw/#176c83d163ea
... A team of five doctors and public health experts found that tort reform measures passed in three states — specifically designed to insulate emergency room doctors from lawsuits — did nothing to reduce the number of expensive tests and procedures those ER doctors prescribed... . . . What they found was that doctors in the tort-reform states – who were virtually immune to malpractice suits – prescribed just as many MRIs and CAT scans as doctors in the control states. Removing the risk of getting sued didn’t change doctor behavior.
According to http://truecostofhealthcare.org/malpractice/ the total yearly outlays for malpractice come to under $10 billion per year. We spend over $3 trillion per year on healthcare, so actual malpractice costs are less than half a percent of medical expenses. This article also discusses "defensive medicine" (AKA ordering a lot of tests) . The doctor there posts his own 2019 malpractice insurance bill:
That’s right, $4,988.02 for the whole year! (It says $5,087.02 because they want a voluntary $99.00 yearly PAC contribution that they add to the the bill.)
The nephrologist who has an office one floor below me pays about $50 a year more than I pay and she runs a dialysis unit.
Also, a pulmonologist I work with pays $6,000- $7,000 a year, an ophthalmologists less than $7,000, emergency room physicians: $11,000-$12,000 a year, anesthesiologists: $12,000-$14,000 a year, surgeons (including orthopedics) $20,000-$22,000 a year and Ob/Gyn about $30,000- $35,000 (obstetrics always has the highest malpractice premiums).













 Source: https://ourworldindata.org/grapher/life-expectancy-vs-health-expenditure
Source: https://ourworldindata.org/grapher/life-expectancy-vs-health-expenditure